Prepare for a long-winded-Katie-authored post. But first a cute kid is pretty excited about her first whole peanut tomorrow!
Now that we’re about half-way through the oral immunotherapy (OIT) treatment, we thought we’d answer some of the questions we've been asked over the last few months – and hopefully now we have pretty good answers. But remember that this is our experience, our perspective, and our daughter – many things will not be exactly the same.
There’s so much to talk about, we’re going to split our Q&A into at least 3 different posts: Diagnosis & Prognosis, Dr.’s Office Questions, and Home Dosing Items. So stay tuned!
Q: "How did you even know she was allergic?"
A: Many people have asked us this question out of concern for their own babies since it never occurred to them to maybe shy away from common allergens with their kids. In case you're wondering, the 8 serious allergens are peanuts, egg, milk, shellfish, fish, tree nuts, soy, and wheat.
We already gave a short timeline of how we figured out what was going on, but here's the more detailed version for those interested.
Family History: Our kid has at least 3 cousins on her maternal side that are allergic to peanuts (and other various things... soy, milk, etc.). Their peanut allergies have not caused significant problems, and they have chosen not to do blood tests. They just avoid anything obviously peanutty. Since we knew it ran in our family, we knew it might be something to look out for.
 First Exposure: After she turned a year old (the advice at the time, and for most mainstream pediatricians, is to wait until the child is at least a year – more on this later), we gave her a peanut butter sandwich. She seemed to like it, no problem. This is how all allergies work. The first exposure doesn't cause any reaction because the body has not made any IgE antibodies against the allergen yet. The cells responsible for making the antibodies needs to "see" the allergen first, then it ramps up IgE production. Check out this site for more information on how food allergies work,
First Exposure: After she turned a year old (the advice at the time, and for most mainstream pediatricians, is to wait until the child is at least a year – more on this later), we gave her a peanut butter sandwich. She seemed to like it, no problem. This is how all allergies work. The first exposure doesn't cause any reaction because the body has not made any IgE antibodies against the allergen yet. The cells responsible for making the antibodies needs to "see" the allergen first, then it ramps up IgE production. Check out this site for more information on how food allergies work,
Second Exposure: A few days later we gave her another peanut butter sandwich. This time she didn't eat all of it, and seemed to have some red itchy looking splotches around her mouth. We thought since there was a family history of peanut allergy we would hold off on the peanuts for another year or so before trying again.
Third Exposure 18 months: While getting a treat one day as a family I unthinkingly gave her a tiny sample cup of peanut butter frozen yogurt. No red splotches this time, just a rash over her entire body! We called our ER doctor brother-in-law and he helped us find the right dose of Benadryl for someone so tiny. She seemed itchy and very crabby from what I remember. But after the Benadryl and a good nap she was fine. At this point we realized this was a real thing, and we needed to see an immunologist.
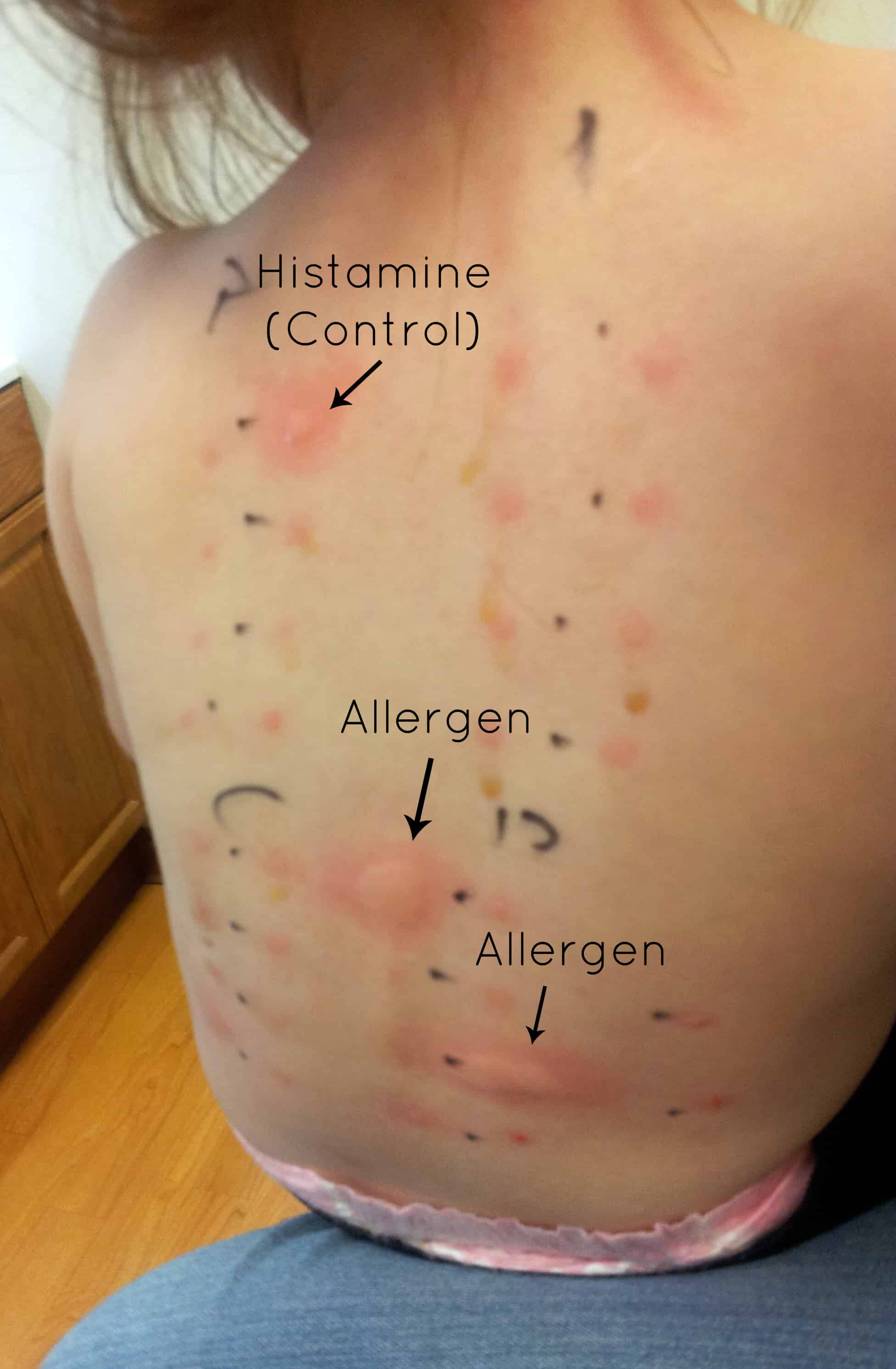 |
| Not our daugther, but similar test |
First Allergist Appointment “Back Scratch Test” – NOT at Dr. Jones Rocky Mountain Allergy and Asthma (RMAA) facility: Here’s a brief description of how a back scratch test is done. For more details on allergy testing go here. They break the skin with just a little scratch, then put the allergen dissolved in a serum onto a little spot. They use straight histamine as a control, to make sure that your body does in fact react to histamine, then use the allergens in question on the rest of the back in a “list” or “grid-like” fashion.
Our daughter was tested against peanuts and other nuts (tree nuts). She was 20 months old, and like any 20 month old she wiggled and squirmed and didn't like what was going on. As luck would have it, the histamine control and the peanut serum dripped down her back a little and ended up all over her arm and side. She screamed HARD for 20 minutes straight. I’d never heard her cry like that (not even with sleep training). We had to hold her arms so that she couldn't scratch anything – she was supposed to be still. We were all absolutely miserable. In retrospect, I should have realized that the part on her arm and side was not normal, and should have had the doctor apply the antihistamine cream to those areas, but I didn't, and we ended up dealing with some long-term consequences. When they finally came in to read the results, the peanut serum had dribbled into the space for almonds, so the Dr. wanted to repeat the test. Um… no way! Instead I suggested that we do the blood test for almond antibodies since we were doing one for the peanut antibody anyway (DUH!). All the other nuts were clear. They finally put the anti-histamine cream on her little tortured back, arm, and side and she fell asleep in my arms almost instantly, completely exhausted. Previously she handled vaccinations and well check visits pretty well, with the normal baby/toddler cry for a minute, then get over it attitude. After the back scratch test, she started crying the second a doctor tried to listen to her heart, refused to stand on the scale just to get weighed, and wailed if any sort of medical instrument was brought within close vicinity. After talking to some other moms at RMAA, I learned that this may have been an abnormal situation – it didn't sound like their kids had been as traumatized.
Blood Tests: Next up we had her blood drawn (another traumatic experience, but it had to be done). Turns out that it was just that the peanut serum did in fact get out of its prescribed circle – she is not allergic to any other nut but peanuts. We do not know if she’s allergic to anything else, as we didn’t have any other immediate concerns and her back was too small to try much else other than nuts at the time. I have absolutely no desire to ever have her do a back scratch test again, but we will likely have to do blood draws every now and then (every 6 months according to this first allergist – haven’t asked the second). The results of her blood tests were described in a previous post, but the take away is that her allergy was getting worse (even with decreased exposure) and that we needed to be prepared for a “very bad” reaction should she ever ingest a peanut – so keep her away from them. Period.
Ever since then, we have been a peanut free home (if only we were allergic to sugar and fat). I haven’t missed it as much as I thought I would – but we’ll both be very happy to have peanut butter cookies again, granola bars, trail mix, Rees’ Peanut Butter Cups………
Q: What is the prognosis for someone with a food allergy?
A: Again, I’m going to be specific to peanut allergies, because that’s what we can speak to. Of all the food allergies, peanuts are the most common cause of food-induced anaphylaxis and hospitalizations. Anaphylaxis is when multiple body systems are responding to the allergen – so you might have any combination of throwing up, rashes/hives, drop in blood pressure, and airway swelling. It’s this airway swelling and drop in blood pressure that are most scary as a person having a reaction can no longer breathe and if not treated right away, can die. If a severe reaction takes place, you treat it with epinephrine. These reactions can occur minutes after exposure, so it is important to have epinephrine with the person who’s allergic at all times – there may be absolutely no time to wait for the paramedics!
 Lindy should have her “Epi-Pen” with her wherever she goes. If we go to the store, we have it (at least in the car). If she’s being babysat, the sitter will get a lesson on how to use the autoinjector. When she’s playing at a friend’s house, her medicine bag goes with her. She has it at preschool. She has it at grandma’s house. She has it with her at all times. We have never had to use it, thankfully, but we try to make sure everyone is prepared should she ever need it. For more information on the “Auvi-Q” epinephrine autoinjector that we use, check out their site. It’s pretty cool!
Lindy should have her “Epi-Pen” with her wherever she goes. If we go to the store, we have it (at least in the car). If she’s being babysat, the sitter will get a lesson on how to use the autoinjector. When she’s playing at a friend’s house, her medicine bag goes with her. She has it at preschool. She has it at grandma’s house. She has it with her at all times. We have never had to use it, thankfully, but we try to make sure everyone is prepared should she ever need it. For more information on the “Auvi-Q” epinephrine autoinjector that we use, check out their site. It’s pretty cool!
Recently there have been some news reports of people who died from allergy-induced anaphylaxis. It got me wondering just how common these kind of deaths are. From my brief time researching, apparently it’s hard to pin down all these allergy numbers. It might be because some people mistake an intolerance for an allergy, or because there are sometimes other factors like asthma that play a role in who reacts more severely. But I feel like it’s a question of when, (not if) Lindy will get exposed. She will. Peanuts are in a vast amount of foods, and in several things you would not automatically think contained peanuts. Here’s a list if you’re curious. That’s why we feel like this is a necessary step for her. That’s why people from around the world have moved to Layton, Utah for a few months, just to be a part of this. It feels like we’re actively diffusing a ticking time bomb! We’re so thankful!



















