This is
purely from our perspective, our experience. These details are specific to our
situation, but would probably be very similar to any other patient looking in
to doing oral immunotherapy (OIT)
 through Dr. Jones at Rocky Mountain Allergy, Asthma,
and Immunology (RMAAI).
through Dr. Jones at Rocky Mountain Allergy, Asthma,
and Immunology (RMAAI).
1.
Q: What’s are the office visits like?
A: The first appointment is just to discuss things
– you as the parent (or patient) decide if this is something you really want to
commit to. The whole process takes about six months. Possibly more depending on if things happen
to throw off the schedule (illness, more severe reactions, etc.). They will order
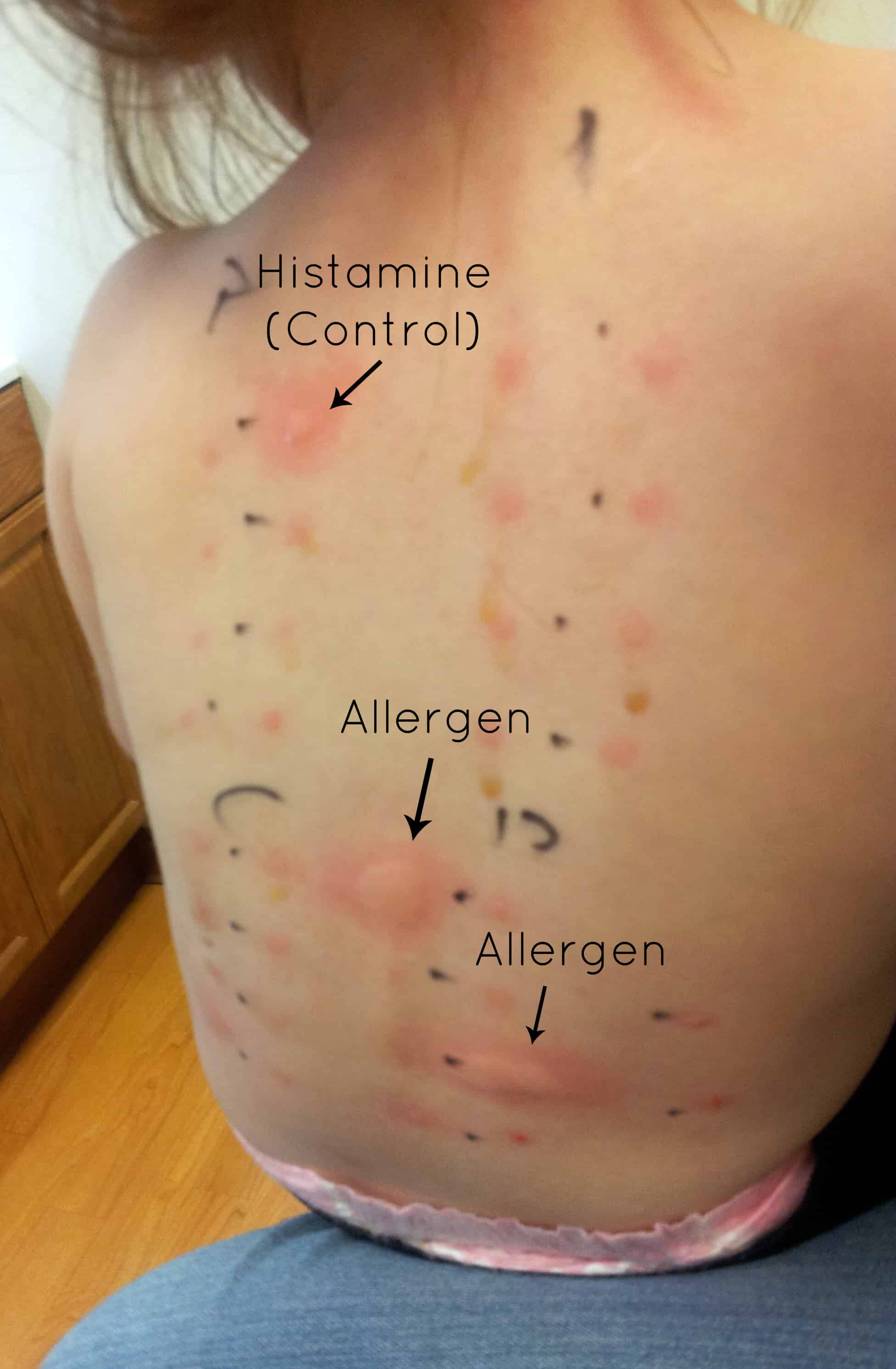
either skin or blood tests to determine the extent of the allergy (we did blood
tests, since we had our documented test results from our previous doctor in
hand for this visit). The first day which I've already described is the
longest. From then on, it means coming
back into the office every week for an "escalation dose" -- meaning
that's where they increase the dose to a new level and monitor for an hour that
there are no problems with the new level of peanut protein in the system. What does this look like in actual
practice? Every week you come to the
office and (1) check in, (2) have the physician or one of his colleagues do a
physical assessment and vitals check, (3) take the new increased dose with the
nursing staff, and (4) sit around in a room in the office for an hour doing
whatever it is you do to entertain a 3 year old (books, trains, Hungry Hungry Hippos,
puzzles, and of course everyone brings their electronic gadgets too). Parents get to chat and talk about all the
things that no one else really understands about the best epi pens, how to
survive at family functions, what you tell their teachers, and so forth. A
reaction to the newly escalated dose is much more likely to happen within the
first hour which is why you get to wait. If there is no problem with the new
dose, they send you on your way with enough of the same dose to do at home for
another week. The dose then escalates again
the following week. No, you are never
increasing the dose at home by yourself, and you still always have the epi-pen
and other meds handy.
2.
Q: What’s the first day of OIT like?
A: The first day of actual treatment is LONG! Check out
Brett’s post about our first day here. You start out taking a teenie tiny dose
of the allergen, then it is doubled every 15 minutes for 5 hours. Brett did the
math and on that first day Lindy consumed 7.6
100ths of a peanut in total. They take this very seriously and start really
slowly. Since you’re there all day you take things to do. We took our computers
for us, and lots of coloring things, books, iPod shows, table games, etc. to do
for Lindy. You also bring snacks and water – they want the stomach to have
something else in it besides the allergen (fruit and crackers was what we did).
The water is for squishing after each dose to make sure it doesn’t linger and
irritate the mouth.
3.
Q: Are there age requirements?
A: The only restriction is that they must be able to physically eat peanuts – so babies are out. His youngest patient was just a little over 3. Our daugther was 3.7ish years old when we started. It very much depends on how “compliant” your kid is. Will he/she take the medicine? Frankly, I was worried about our squirt on this one – still am a bit. She’s up to eating real peanuts now, but doesn’t love them, so it’s sometimes hard to get her to want to eat them (chocolate is helpful here). Dr. Jones says he thinks younger patients handle their anxiety about treatment better; it’s harder for older kids who understand that they could have a reaction to remain calm while eating peanuts. He has a lot of children and adolescents as patients, but has a growing number of young adults 18-25. His oldest patient is a 65 year old physician who has had many anaphylactic episodes during his life and he’s ready to be done worrying about it! Everything seems to be working the same for him as for the kids!
A: The only restriction is that they must be able to physically eat peanuts – so babies are out. His youngest patient was just a little over 3. Our daugther was 3.7ish years old when we started. It very much depends on how “compliant” your kid is. Will he/she take the medicine? Frankly, I was worried about our squirt on this one – still am a bit. She’s up to eating real peanuts now, but doesn’t love them, so it’s sometimes hard to get her to want to eat them (chocolate is helpful here). Dr. Jones says he thinks younger patients handle their anxiety about treatment better; it’s harder for older kids who understand that they could have a reaction to remain calm while eating peanuts. He has a lot of children and adolescents as patients, but has a growing number of young adults 18-25. His oldest patient is a 65 year old physician who has had many anaphylactic episodes during his life and he’s ready to be done worrying about it! Everything seems to be working the same for him as for the kids!
4.
Q: What if my allergy is worse than yours? Is it
safe?
A: You can see our girl’s blood work on this post.
She’s anaphylactically allergic to the 3 peanut proteins. However, she has
never reacted to anything processed in a factory that processes peanuts or
reacted to the smell of peanuts in a room, so I’m sure there are kids who are
more sensitive than she is. However, it is those super sensitive kids who need
this treatment the most, since completely avoiding a peanut particle floating
in the air for the rest of their lives is very unlikely! We’ve heard other
parents say that their doctors do not recommend this treatment. But I think
they need to think about the source of that information for a second. While I’m
sure that they care about your child as a patient, they also aren’t likely to
recommend you leave their office to be treated somewhere else (can you say “conflict
of interest?”). They might say, “It’s not safe!” And that’s true – it isn’t
safe to do it in THEIR office – they do not have the protocols in place, nor
the experience needed to offer this program safely. Dr. Jones does! They are
ready for the worst. If someone were to have an anaphylactic episode in the
office, they are prepared to intubate and stabilize before rushing over to
Davis hospital which is a parking lot away. They have never had to do that.
They have had to give their cocktail of antihistamines (described in the next
post), and they have had to do epinephrine injections, but they’ve never had to
intubate. Even those who had reactions continued on, and have “graduated” the
program. I know we sound like we’ve been paid to advertise for him, but the
results advertise for themselves! My anaphylactically allergic kid is eating
peanuts! Our old allergist would never have been able to do that for us. For
those who have been told not to try this treatment, please at least talk to Dr.
Jones, go to one of his seminars, or check out the news reports – it can’t hurt.
There are kids who have had serious reactions in the past who have graduated or
who are currently in this program – you are not alone!
5.
Q: How can they do this so quickly? Do they do
this for seasonal allergies?
A: I’m not sure how the biology works, but
something about actually ingesting the allergen and building up the tolerance
that way is actually quite fast. In fact other allergens can be treated even
faster! The milk allergy program is done in 4 months (I think), while peanut
takes 6. But still… 6 months of weekly visits for a lifetime of freedom… um…
YES! For seasonal allergies they do allergy shots just like other offices. I’m
guessing the time frame and treatment plan will differ from person to person,
and I don’t know if it’s any quicker at his office than any other. We have
seasonal allergies, but are attacking the peanut at the moment.
6.
Q: Does insurance cover it?
A: This probably depends on your insurance company.
We have Select Health and immunology is covered once we hit our deductible.
However, you will want to double check with your insurance company to make sure
RMAAI (aka. Dr. Douglas Jones) is covered by your plan. Before treatment begins
they will get all your insurance information and determine how everything will
be paid – they want to make sure they get paid, just like any other business.
So if your insurance company doesn’t cover this, I’m pretty sure you’ll find
out early on. Billing happens once a month even though you are incurring costs
every week. They are billed like a
normal physician office visit in our case.
7.
Q: How can I learn more?
A: Here is a link to RMAAI website. You'll probably be interested in some of the videos on the website too if you're interested.
A: Here is a link to RMAAI website. You'll probably be interested in some of the videos on the website too if you're interested.